For payers, carriers, and claims professionals, that pressure lands squarely on claims infrastructure. Legacy systems that separate medical and pharmacy data create coordination gaps, delayed adjudication, and missed cost-control opportunities — at a scale the industry can no longer afford.
Integrated PBM systems are the structural response. By unifying pharmacy and medical claims into a single platform, they change how data flows, how costs are managed, and how organizations detect fraud. This article covers what PBM integration actually means, how it reshapes claims workflows, the concrete benefits for payers and employers, its impact on fraud detection, and what growing data complexity means for defense and claims teams navigating the results.
Key Takeaways
- Integrated PBM systems consolidate medical and pharmacy claims into one platform, eliminating the coordination gaps that siloed arrangements create
- Daily accumulator file syncing closes the "real-time" lag between prescription fills and medical claim posting
- A peer-reviewed study found carve-in members had $8.73 lower PMPM medical costs versus carve-out arrangements
- Unified claims data strengthens fraud detection by correlating prescription records with diagnosis codes
- Integrated PBM files are substantially larger and more complex, making AI platforms essential for managing the defense review burden
What Is an Integrated PBM System?
The PBM Role
As KFF defines it, Pharmacy Benefit Managers act as intermediaries between insurers, drug manufacturers, and pharmacies to manage prescription drug benefits. In practice, a PBM:
- Adjudicates pharmacy claims by verifying eligibility and formulary coverage
- Negotiates drug pricing and rebates with manufacturers
- Manages formularies on behalf of health plans and employers
- Administers prior authorizations for specialty and high-cost medications
PBMs don't provide care — they sit in the financial and administrative layer between the parties who do.
Integrated vs. Carved-Out: What's the Difference?
Employers and plan sponsors have two structural options. A carve-out arrangement uses a separate PBM to administer pharmacy benefits independently from the insurer managing medical benefits. A carve-in (integrated) arrangement administers both through the same vendor or platform.
That structural distinction has real consequences for claims teams:
| Feature | Carved-Out | Integrated (Carve-In) |
|---|---|---|
| Data flow | Separate systems, manual reconciliation | Single unified platform |
| Claims adjudication | Independent workflows | Simultaneous cross-check |
| Care coordination | Coordination gaps | Unified member view |
| Fraud detection | Partial visibility | Correlated across benefit types |
| Reporting | Multiple data sources | Single source of truth |
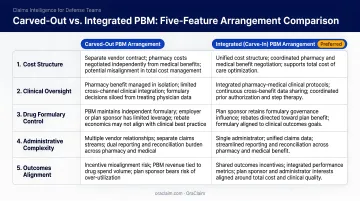
With carved-out arrangements, medical and pharmacy data live in separate systems. Identifying a drug interaction requires pulling records from two vendors. Catching duplicate billing across benefit types requires manual cross-referencing. Integration eliminates that divide.
How Integrated PBM Systems Reshape Claims Processing
From Fragmented to Unified Adjudication
In legacy systems, medical and pharmacy claims run through separate workflows. A prescription fill generates a pharmacy claim; a physician visit generates a separate medical claim. Neither system sees the other in real time, which creates redundant tasks, delayed cross-referencing, and missed optimization opportunities — particularly for high-cost chronic disease patients whose drug utilization directly affects medical utilization.
Integration enables simultaneous adjudication. When a pharmacy claim is processed, the system can check it against diagnosis codes, prior authorization records, and benefit accumulators in the same pass.
The "Real-Time" Nuance
"Real-time" in PBM contexts deserves clarification. The NCPDP Telecommunication Standard supports pharmacy claim responses within seconds — that part is genuinely fast. But a member may fill a prescription before their related medical claim is even submitted, let alone posted. This lag creates accumulator discrepancies where members appear to have more remaining benefit than they actually do.
Integrated systems close this gap using daily accumulator files that sync data between PBMs and TPAs. These files keep benefit accumulators current across both medical and pharmacy sides, preventing members from being overcharged and preventing plan overpayments.
TPA-PBM Coordination
Modern integrated PBMs can now:
- Send and receive daily claims files to TPA partners automatically
- Grant TPA clients real-time system access to monitor claims flow
- Share prior authorization data and methodology directly with TPAs
This gives TPAs the tools to service employer groups without depending on large integrated carrier plans, a direct advantage for self-insured and mid-market employers building independent administrative infrastructure.
The Administrative Cost Opportunity
CAQH's 2023 Index put the industry-wide savings opportunity from fully electronic administrative transactions at $18.3 billion — rising to $21 billion in the 2025 Index. Administrative complexity already accounts for roughly $400 billion, or 10% of total U.S. healthcare expenditures.
Fewer manual touchpoints mean faster processing, fewer errors, and reduced staff burden. A McKinsey analysis of payer automation found payers could achieve 13% to 25% net administrative-cost savings using currently available technology.
Carve-In vs. Carve-Out: The Cost Evidence
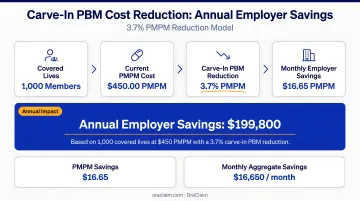
The strongest independent comparison comes from a 2020 JMCP peer-reviewed study of a regional health plan, which found that carve-in members had $8.73 lower PMPM medical costs — a 3.7% reduction — compared to carve-out members. Carve-in members also showed 4.9% higher participation in insurer-based health management programs.
For a self-insured employer covering 5,000 members, that $8.73 PMPM difference translates to roughly $524,000 in annual medical cost reduction before accounting for any pharmacy-side savings.
Key Benefits for Payers, Carriers, and Employers
Care Coordination and Readmission Reduction
When providers and payers share a unified view of a member's medical and prescription history, care gaps close faster. A 2021 peer-reviewed review found that 16% of 30-day readmissions were medication-related, with 40% of those considered potentially preventable. A subsequent scoping review cited a meta-analysis showing pharmacist-led medication reconciliation reduced readmissions by 19%.
Integrated claims data is what makes proactive medication reconciliation possible at scale — without it, the data lives in separate systems that don't talk to each other.
Medication Adherence Monitoring
Integrated platforms let payers identify members who aren't following prescribed treatment regimens early enough to intervene. This matters financially. A widely cited PMC review estimates the annual cost of medication non-adherence to the U.S. healthcare system at $100 billion or more when direct and indirect costs are included.
The mechanism is straightforward: when pharmacy fill data sits alongside medical utilization data, gaps in adherence become visible. Without integration, a plan might see the downstream medical costs without ever connecting them to unfilled prescriptions.
Medication Therapy Management (MTM)
Adherence gaps feed directly into a broader clinical challenge: ensuring patients are on the right therapies in the first place. Integrated claims data enables more effective MTM programs by giving clinicians a complete picture — not just a pharmacy snapshot. MTM programs include comprehensive medication reviews, patient education, and adherence support. CMS has specifically tested whether additional payment incentives tied to MTM would improve therapeutic outcomes while lowering Medicare expenditures, recognizing that claims data completeness directly affects program effectiveness.
Predictive Analytics for Population Health
MTM programs address individual members — but unified data enables action at the population level too. Predictive models can identify high-risk patients before costs escalate. The healthcare analytics market reflects this demand: one market report projects growth from $69.74 billion in 2026 to $213.27 billion by 2031.
Specific applications include:
- Flagging members with high-cost chronic conditions before hospitalizations occur
- Spotting utilization trends that signal emerging population health risks
- Guiding targeted clinical interventions for defined member cohorts
- Informing plan design decisions based on actual utilization patterns
Single Source of Truth for Plan Administration
Integration simplifies reporting by creating one authoritative data record across all benefit types. This reduces reconciliation work, supports accurate regulatory filings, and gives employers clearer visibility into total cost of care — without assembling data from two separate vendors whose records don't always align.
How PBM Integration Strengthens Fraud Detection and Compliance
The Scale of the Problem
The FBI states that healthcare fraud costs the industry tens of billions of dollars annually. In 2024 alone, the DOJ charged 193 defendants in schemes involving more than $2.75 billion in alleged false claims.
Siloed data makes this problem harder to catch. Each system only sees a portion of a member's activity — a pharmacy system sees fills but not diagnoses; a medical system sees encounters but not prescription patterns. That partial visibility is exactly what bad actors exploit.
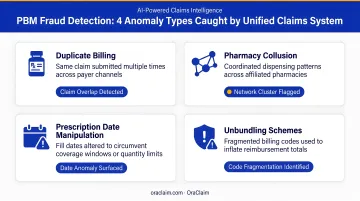
Anomaly Detection Across Benefit Types
When prescription data is correlated with diagnosis codes in a unified system, organizations can identify:
- Inappropriate prescribing patterns — medications filled without supporting diagnoses
- Duplicate therapies from multiple prescribers, often across different pharmacies
- Billing inconsistencies that span both medical encounters and pharmacy claims
- Duplicative claim reimbursements — CMS specifically notes that online adjudication of prescription drug claims limits this type of fraud
Embedded rules engines act proactively, flagging anomalies before payments are made rather than after. That upstream intervention is where integrated systems deliver their clearest financial return.
Compliance and PHI Protection
That same integration that improves fraud detection also tightens compliance posture. When medical and pharmacy data are harmonized in a single environment, the PHI footprint shrinks — and so does the attack surface.
For carriers and payers managing large covered populations, this consolidation produces concrete compliance advantages:
- Fewer PHI touchpoints reduce data vulnerability exposure across the organization
- Stronger access controls become easier to enforce with one environment instead of many
- Simpler security oversight lowers the administrative burden of HIPAA audit readiness
- Clearer governance around HHS business associate obligations, which apply to PBMs and integrated platforms that use or disclose PHI for covered entities
Governance clarity here isn't just a best practice — it's a compliance requirement.
What Integration Means for Defense and Claims Professionals
Larger, More Complex Data Sets
Integrated PBM systems are a net positive for health plan operations. For defense teams, however, they create a different challenge: when claims are disputed or litigated, the data universe has expanded substantially.
A single litigated claim may now span:
- Medical records across multiple providers and specialties
- Prescription histories from integrated pharmacy benefit files
- Prior authorization trails and denial records
- Benefit accumulator data showing how cost-sharing was applied
- PBM adjudication records for disputed claims
Without the right tools to structure that volume, manual review becomes a serious bottleneck.
The Unstructured Data Problem
Integrated PBM systems aggregate information from disparate sources, and much of it arrives in inconsistent formats. Pharmacy records, medical records, and benefit administration data don't share a common structure.
For claims professionals managing high volumes of disputed or litigated files, parsing this data manually creates significant review burden. Looking for the prescription non-compliance that undermines a causation argument, or the prior authorization denial that affects coverage, carries real risk of missing critical facts.
How AI Platforms Support Defense Teams
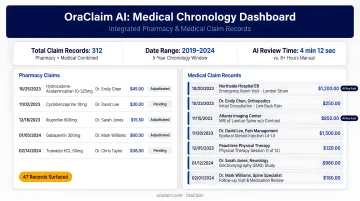
This is where AI tools purpose-built for defense workflows make a concrete difference. OraClaim's claim file review and medical chronology capabilities ingest entire claim files (medical records, pharmacy records, ER reports, specialist notes, imaging reports, and treatment documentation), automatically classify every document, and surface the findings that drive exposure and liability.
For files that include pharmacy records alongside medical documentation, OraClaim's medical chronology module builds chronological summaries with dedicated medication columns, flags treatment gaps and non-compliance patterns, and identifies inconsistencies between subjective complaints and documented prescription fills. The case evaluation module synthesizes across all record types (including pharmacy data) to generate comprehensive exposure analysis in minutes rather than the 10–40 hours that manual review typically requires.
As PBM-integrated claim volumes grow and data complexity increases, the ability to systematically structure and interrogate that data separates defense firms and claims organizations that stay ahead from those buried in manual review.
The Future of Integrated PBM and AI-Driven Claims
AI-Powered Decision Support at the Point of Care
As integration matures, AI moves beyond process automation into prescriptive decision support. Near-term capabilities include real-time benefit checks at the pharmacy counter, contraindication flags before prescriptions are filled, and personalized formulary recommendations drawn from a member's complete claims history. The infrastructure for this already exists in integrated platforms — the AI layer is what turns data connectivity into actionable guidance.
The Value-Based Care Connection
PBM integration is foundational to value-based care models. The 2024 HCP-LAN APM report found that 45.2% of healthcare payments were already flowing through value-based arrangements (Categories 3–4 APMs) for CY 2023. Those arrangements require connecting drug utilization directly to measurable clinical outcomes — which requires the kind of data connectivity that integrated PBM platforms provide.
Without it, shared savings calculations and risk allocation rest on incomplete data — and when disputes arise over those calculations, the downstream claims and litigation complexity multiplies. For carriers, TPAs, and the defense organizations handling those disputes, the data gaps that emerge upstream translate directly into harder-to-defend claims downstream.
What Forward-Looking Organizations Should Prepare For
Organizations investing in integrated PBM infrastructure and AI analytics now will be better positioned as:
- Benefit types, data sources, and adjudication touchpoints multiply — making unified records a baseline requirement, not an advantage
- Regulatory scrutiny intensifies around value-based metrics, formulary compliance, and audit readiness
- Claim volumes increase as aging populations and chronic disease prevalence drive sustained pharmacy utilization growth
- Disputes over benefit determinations and claims outcomes become more complex, raising the stakes for defense-side preparedness
For payers, carriers, TPAs, and the defense organizations that manage their claim disputes, this is a strategic readiness question. The organizations that build AI-powered claims intelligence into their workflows now — surfacing facts faster, benchmarking exposure earlier, and managing portfolio risk proactively — will be far better positioned when claim complexity catches up with them.
Frequently Asked Questions
Do PBMs process claims?
Yes. PBMs process pharmacy claims on behalf of health plans and employers, adjudicating each prescription by verifying member eligibility, confirming formulary coverage, and calculating the correct cost-sharing before authorizing the pharmacy to dispense. Most transactions are completed within seconds under the NCPDP standard.
What is pharmacy benefits management software?
It's the technology platform PBMs use to administer prescription drug benefits, covering claims adjudication, formulary management, prior authorizations, eligibility checks, rebate processing, and reporting for health plans, employers, and TPAs. Integrated versions extend this into unified medical-pharmacy platforms that consolidate data across both benefit types.
What is the difference between integrated and carved-out pharmacy benefits?
Integrated (carve-in) pharmacy benefits are administered through the same vendor managing medical benefits, enabling unified data flow. Carved-out arrangements use a separate PBM, which can offer pricing flexibility but creates coordination gaps and data silos between medical and pharmacy claims.
How does PBM integration reduce fraud and waste?
By correlating prescription data with medical diagnosis codes in a single system, integrated PBMs detect anomalies that siloed systems miss: inappropriate prescribing, duplicate therapies, and billing inconsistencies. This enables real-time intervention rather than after-the-fact recovery.
How does integrated claims data benefit insurance carriers and payers?
Carriers and payers gain a complete, auditable view of member health utilization. That unified picture supports more accurate plan pricing, stronger fraud controls, faster regulatory reporting, and better disease management — all without reconciling data across separate medical and pharmacy vendors.
What role does AI play in integrated PBM systems?
AI automates claims adjudication, detects fraud patterns in real time, and generates predictive risk models for high-cost members. For defense and claims teams, it also rapidly extracts and structures critical insights from complex, unified claims datasets — converting raw data volume into measurable decision-making value.