Automating medical record review sounds simple. In practice, results vary widely based on tool selection, workflow configuration, data preparation, and how human oversight is structured.
This guide covers what automation actually involves, the exact steps to implement it for insurance claims, the variables that drive results, and the mistakes that cause most rollouts to fail.
Key Takeaways
- Manual medical record review is expensive, inconsistent, and unsustainable at high caseload volumes
- Effective automation uses four technologies in sequence: OCR, NLP, AI-based extraction, and confidence-tiered routing
- Preparation determines whether deployment succeeds or stalls: data infrastructure, workflow mapping, and compliance architecture matter most
- Common failure points: skipping baseline measurement, deploying general-purpose tools, and expecting full automation without human oversight
- Purpose-built claims-defense platforms reach time-to-value faster than adapted document processing tools
Why Manual Medical Record Review Fails Defense Teams
Medical records don't arrive in a standard format. A single claim file might contain scanned handwritten physician notes, structured lab exports, faxed hospital discharge summaries, and imaging reports, each requiring a different extraction approach. Standardizing that mix manually, at volume, isn't realistic.
A CLM Magazine article on unstructured claims data notes that 80% of company data is unstructured and 90% of that information is unmanaged. Medical records sit among the most complex unstructured data defense teams handle.
The Compounding Cost Problem
Manual extraction creates expensive downstream problems:
- Repeated review cycles when initial extraction misses key clinical details
- Reserve surprises from treatment inconsistencies or causation gaps discovered late
- Quality variation when temporary staff handle high-volume periods
- Senior counsel pulled into document review so high-cost time gets applied to low-skill tasks

OraClaim's founders, Mark Tepper and Andy Anderson, observed this directly while litigating claims and managing high-exposure cases. They saw manual document review absorb large blocks of associate time without producing strategic analysis, reserve insight, or litigation-ready work product.
The Compliance Problem
Audit trails (records documenting what was reviewed, what was extracted, and how decisions were made) are difficult to maintain consistently through manual processes. The NAIC Market Regulation Handbook establishes that claim files must be adequately documented, accessible, and consistent. Manual workflows create regulatory exposure precisely because they can't produce that documentation reliably under examination.
What You Need Before Automating Medical Record Review
Automation works only as well as the records, systems, and controls behind it. If you deploy AI before those pieces are ready, accuracy drops at scale, compliance gaps widen, and integration problems can wipe out the expected efficiency gain.
System and Workflow Requirements
Before selecting any platform, confirm your existing tech stack supports integrations. Automation tools that can't connect to your practice management or document management systems force context-switching and manual data re-entry, which eliminates much of the expected efficiency gain.
OraClaim integrates with Clio, MyCase, Smokeball, PracticePanther, NetDocuments, iManage, Worldox, and Box. Confirm similar compatibility before committing to any platform.
Compliance and Security Readiness
For insurance defense and claims teams, two frameworks usually control AI-assisted medical record review:
HIPAA Business Associate obligations:
- Any platform processing protected health information (PHI) on behalf of a covered entity must operate under a Business Associate Agreement
- HHS requires BAAs to establish permitted uses, safeguards, breach notification, and subcontractor obligations
- 45 CFR 164.308 requires documented risk analysis covering threats to electronic PHI confidentiality, integrity, and availability
NAIC Model Bulletin on AI Systems:
- Adopted December 4, 2023; verify current adoption and guidance in each claims jurisdiction
- Scope explicitly includes claim management, claim administration, and payment
- Requires a written AI Systems Program, documented data practices, predictive model inventories, and evidence of regular model validation and drift assessment
- During examination, regulators may request data sources, validation results, and third-party vendor contracts including audit rights
Verify your chosen platform meets these requirements before processing any PHI.
How to Automate Medical Record Review for Insurance Claims
Step 1: Audit and Document Your Current Review Workflow
Map how medical records currently move through your organization, from intake through extraction, review, and decision. Identify where bottlenecks, errors, and rework cycles concentrate.
Establish baseline metrics before deployment:
- Processing time per record type
- Error rates by document category
- Exception and escalation rates
- Average cost per reviewed case
Without these baselines, you cannot measure ROI, identify which document types benefit most from automation, or justify continued investment internally.
Step 2: Select an AI Platform Built for Defense and Claims Use Cases
Evaluate platforms on four criteria:
- Multi-format document ingestion: handles PDFs, handwritten notes via OCR, structured EHR exports, and fax-originated records
- Confidence scoring: routes uncertain extractions to human reviewers rather than passing them through unchecked
- Integration depth: connects directly with your case management or practice management systems
- HIPAA-compliant audit trail generation: logs every access, extraction, and decision natively
General-purpose document tools do not understand clinical terminology in the context of claims defense. They cannot surface treatment gaps as causation red flags, flag inconsistencies between subjective complaints and objective findings, or identify pre-existing conditions relevant to comparative fault analysis.
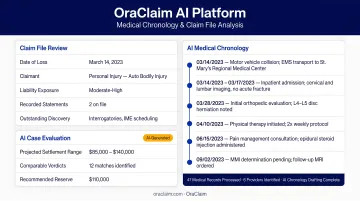
Platforms like OraClaim are built specifically for defense lawyers and claims professionals. The AI automatically ingests entire claim files, including medical records, demand packages, police reports, expert reports, depositions, and correspondence. It classifies every document, extracts clinically relevant facts, and produces litigation-ready work product such as medical chronologies, key fact summaries, and anomaly flags. Medical chronology drafting time drops from 15–60+ hours per file to under 60 minutes for a first draft.
Step 3: Structure Your Document Intake and Classification Process
Configure the system to ingest records from all incoming channels: provider portals, fax, email, and health information platforms. The classification engine should automatically recognize and sort document types without manual routing.
Key structured data elements to extract for claims defense:
- Diagnosis codes (ICD-10) and procedure codes (CPT)
- Treatment histories with dates and provider identifiers
- Medication lists and pharmacy records
- Treatment gaps and missed appointments
- Pre-existing conditions, prior accidents, comorbidities
- Inconsistencies between subjective complaints and objective findings
- Billed vs. paid amounts for medical specials calculation
Each extracted element should be citation-linked back to the source document page for cross-examination preparation and deposition use.
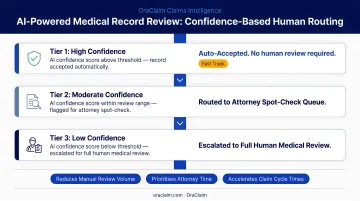
Step 4: Deploy Confidence-Tiered Routing for Human-AI Review
Not every extraction warrants the same level of human attention. A three-tier model allocates reviewer time efficiently:
| Tier | Confidence Level | Processing Path |
|---|---|---|
| Tier 1 | High | Straight-through processing, no human review required |
| Tier 2 | Mid-range | Automated extraction with quick human validation |
| Tier 3 | Low | Full expert review with AI-generated summaries as support |
Define confidence thresholds based on your organization's error tolerance and the cost of missed clinical details. Start conservative during the pilot phase, with lower thresholds and more human review, then raise them incrementally as accuracy is validated across document types. Revisit thresholds at 30, 60, and 90 days into production.
Step 5: Monitor, Measure, and Refine Continuously
Track KPIs from day one:
- Records reviewed per hour
- Extraction accuracy on key clinical fields
- End-to-end cycle time per case
- Rework and escalation rates
Use performance data to identify where the model needs improvement. Establish regular review cycles, monthly at minimum, where extraction quality is assessed against the baseline metrics established in Step 1. This is how you demonstrate ROI and identify which document types or record sources generate the most exceptions.
Key Variables That Affect Automated Review Results
Automation performance is not fixed. Four controllable variables determine whether results improve or plateau.
Document Quality and Standardization
AI extraction accuracy drops quickly with low-resolution scans, heavy handwriting, or non-standard formats. Document quality is the single largest driver of confidence score variation.
Set minimum digitization standards for incoming records: resolution requirements, accepted file formats, and legibility checks. Then run documents through quality gates before they enter the extraction pipeline.
Confidence Threshold Configuration
Setting thresholds too high floods human reviewers with unnecessary escalations. Setting them too low allows errors through straight-through processing. Start conservative, validate accuracy across document types, then raise thresholds incrementally. The right calibration depends on your error tolerance and the claim impact of a missed clinical detail.
Integration Depth with Case Management Systems
Automation that operates in a silo loses efficiency gains to context-switching and manual data re-entry. Before committing to a platform, confirm:
- Which specific systems it connects with
- Whether sync is bi-directional or one-way export
- Whether extracted data flows automatically into case records or requires manual transfer
The difference between deep integration and surface-level connectivity determines whether your team actually saves time or simply shifts where the manual work happens.
Compliance Architecture
Platforms that do not include native HIPAA audit trails and AI governance documentation create compliance debt that compounds over time. Verify before going live that your platform:
- Logs every access, extraction, and decision with timestamps and user identification
- Generates audit trail records in formats acceptable under applicable jurisdiction requirements
- Supports the documentation required under the NAIC Model Bulletin if you operate in any of the 25 adopting states
Common Mistakes When Automating Medical Record Review
Skipping baseline measurement before deployment. Without documented current-state metrics, teams cannot quantify ROI, isolate the document types with the biggest gains, or defend the investment when results are challenged.
Treating automation as a replacement for human expertise. The most effective model uses AI for high-volume extraction while keeping attorneys, adjusters, and nurse reviewers focused on risk assessment, exceptions, and strategic decisions. Deployments that try to eliminate human review create accuracy and compliance problems.
Deploying a general-purpose document AI instead of a defense-specific platform. Generic tools do not understand clinical terminology in claims-defense context, surface coverage-relevant facts reliably, or provide the HIPAA-compliant audit trails regulated teams need. A defense-specific platform closes that gap when it is built for claim file review, not repurposed from plaintiff intake or generic document processing.
Frequently Asked Questions
What are the 5 C's of medical record documentation?
The commonly cited 5 C’s are Client-centered, Clear, Concise, Complete, and Correct. For automated review, completeness and clarity matter most because vague or missing documentation lowers AI confidence and sends more items to human review.
How long does it take to review 300 pages of medical records?
There is no universal benchmark, but AALNC attorney testimonials reference 8–10 hours for one complex record review. For comparison, OraClaim reduces medical chronology drafting from 15–60+ hours per file to under 60 minutes for a first draft.
Is automated medical record review HIPAA compliant?
Automated review can be HIPAA compliant if the platform is built for PHI handling. Before use, confirm a Business Associate Agreement, audit trails, access controls, and documented risk analysis under 45 CFR 164.308.
What types of medical records can AI review for insurance claims?
AI can review lab reports, physician notes, prescription histories, imaging summaries, EHR exports, discharge records, ER reports, surgical reports, therapy records, and EMS records. Handwritten notes usually need stronger OCR and may receive lower confidence scores than structured digital files.
How is automated medical record review different from manual review?
Manual review depends on individual expertise and available staff time. Automated review applies consistent extraction logic, flags exceptions for human review, and produces auditable outputs at higher volume without a matching increase in cost.
What should defense teams look for when selecting a medical record review automation platform?
Prioritize HIPAA-ready audit trails, confidence-tiered routing, integration with practice or claims systems, and defense-specific workflows. A platform purpose-built for insurance defense, such as OraClaim, can evaluate medical facts in the context of coverage, causation, and comparative fault.